Nov 13, 2025
Referring physician meaning: A Clear Guide to Your Care
Discover the referring physician meaning and how it shapes your care, with tips to identify their role in your journey.
At its core, a referring physician is the healthcare provider who sends a patient to another clinician—usually a specialist—for diagnosis or treatment. But that simple definition doesn't capture the immense influence they have. This one action is the first critical domino to fall, setting in motion the patient’s entire treatment path.
The True Meaning of a Referring Physician

Forget the dry, dictionary-style definition for a moment. The best way to understand the role of a referring physician is to think of them as the ‘quarterback’ of a patient's care team. Their job isn’t just to hand off the patient and walk away; it's to make the strategic decision that directs the entire course of treatment.
A classic practical example is a primary care physician (PCP) who detects an unusual heart rhythm during a routine check-up. When they send that patient to a cardiologist for a deeper evaluation, they are acting as the referring physician. They've just initiated a crucial new phase of care, yet they remain the central figure in that patient's long-term health story.
More Than Just a Hand-Off
This role is fundamentally about ensuring continuity of care. When a patient's needs go beyond a generalist's scope, the referring physician acts as a critical gatekeeper, connecting them to the right specialized services. They are providing essential oversight, making sure that any specialist interventions make sense within the context of the patient's broader medical history and health goals. You can explore more on the formal role in a glossary entry from Definitive Healthcare.
Without this coordinated effort, patients could easily get lost in the system, leading to fragmented care, frustrating delays, and ultimately, poorer outcomes.
Key Takeaway: The referring physician doesn't just pass a patient along. They identify a specific need, select the appropriate specialist or facility, and set the entire downstream care process in motion. This makes them a primary influencer of a patient’s treatment pathway.
Referring Physician vs Other Physician Roles
The healthcare ecosystem is filled with different physician designations, and it's easy to get them mixed up. "Referring physician" actually describes a specific function a doctor performs, not necessarily their job title. A single clinician can wear multiple hats, but understanding the differences is absolutely critical for any life sciences team trying to map out patient journeys.
Getting these roles right isn't just an academic exercise—it has major real-world consequences. For example, as noted by NC Medicaid, billing claims must correctly identify whether the provider was rendering, attending, ordering, or referring. Misidentifying the role can lead to rejected claims and compliance headaches.
To help clear things up, let's compare these distinct functions.
Referring Physician vs Other Physician Roles
Physician Role | Primary Function | Key Responsibility |
|---|---|---|
Referring Physician | To direct a patient to another provider for specialized care. | Initiating the care pathway and connecting the patient to the right specialist. |
Attending Physician | To have overall responsibility for a patient's care in a hospital setting. | Supervising medical students and residents; making final treatment decisions. |
Prescribing Physician | To authorize medications for a patient. | Writing prescriptions and managing a patient's medication regimen. |
Ordering Physician | To request tests, procedures, or medical supplies. | Authorizing diagnostic imaging, lab work, or durable medical equipment (DME). |
As you can see, while an attending physician in a hospital might also order a CT scan and prescribe medication, the referring physician is the one who started the patient on that path in the first place. For commercial teams, this distinction is everything.
The Evolution of Physician Referral Patterns
To really understand what a referring physician does today, you have to look at how much the referral game has changed. Physician networks aren't some static, old-boys' club. They're dynamic, living ecosystems, and the simple act of one doctor sending a patient to another has become a much bigger, more frequent part of the business of healthcare.
This isn't just a gut feeling; the data tells a clear story. Landmark research that tracked a full decade of physician activity showed a stunning jump in referral rates. Between 1999 and 2009, the odds that any given office visit would end in a referral nearly doubled, climbing from 4.83% to 9.29%.
While that might sound like a small shift, the real-world impact was enormous. The total number of patient visits that led to a referral skyrocketed from 40.6 million to 105 million in that ten-year span—a 159% surge nationwide. You can dig into the full research about this referral boom to see the numbers for yourself.
What Caused This Referral Boom?
So, what was behind this massive shift? It wasn't one single thing. Instead, a few powerful trends came together, making referrals not just more common, but often essential. Getting a handle on these drivers is the key to seeing why the referring physician has become such a pivotal figure.
A few key factors were at play:
Deeper Specialization: Medicine has become incredibly specialized. It's no longer enough to see a cardiologist. Now, a general cardiologist might send a patient with a heart rhythm problem to an electrophysiologist—a specialist within a specialty.
The Maze of Insurance Networks: The rise of managed care plans like HMOs and PPOs brought a new layer of complexity. These plans often have strict rules about which specialists a patient can see, forcing the referring physician to act as a navigator.
New Ways of Delivering Care: The growth of Accountable Care Organizations (ACOs) and other models focused on value put a huge premium on coordinating care. Formal referrals became a structural requirement for making sure everyone was on the same page.
A referral is no longer just a simple recommendation. It’s a critical transaction that directs the flow of patients—and billions in healthcare spending. As referrals go up, so does the use of the expensive diagnostics, devices, and drugs that specialists provide.
For commercial teams in pharma and medtech, this history lesson is incredibly important. It points to a clear strategic truth: the doctor who makes the initial referral often holds the keys to the kingdom. They are the gatekeepers to the high-value specialists your sales teams are trying to reach, and understanding their influence is the first step toward finding new growth opportunities.
Why Referring Physicians Are Your Commercial Blind Spot
Most life science commercial teams have a laser focus on high-volume surgeons and specialists. On the face of it, this is a sound strategy—they’re the ones actually performing the procedures or prescribing the drugs. But it also creates a massive blind spot, because it means you’re only seeing the end of the patient journey, not where it began.
Imagine the healthcare ecosystem as a vast river. The downstream specialist—say, an interventional cardiologist or a surgical oncologist—is that wide, powerful main channel where a specific treatment happens. Commercial teams understandably spend most of their time and resources right there.
But where does all that water come from? It flows from countless smaller streams and tributaries. In this landscape, referring physicians are the tributaries. They are the PCPs, general cardiologists, and other frontline clinicians who control the patient flow, deciding exactly which "river" each patient ends up in.
The Upstream Decision That Shapes Everything
That initial choice made by the referring physician determines which specialist a patient sees. That, in turn, heavily influences which drugs, devices, or diagnostics are ultimately used. It's an upstream decision with huge downstream consequences for your product.
By the time a patient arrives at the specialist you're targeting, the key opportunity to influence their journey might already be gone.
Think about a patient who goes to their PCP with symptoms of atrial fibrillation (AFib). That PCP's referral is a critical fork in the road.
Practical Example (Path A): The PCP refers the patient to a cardiologist who primarily relies on novel anticoagulants to manage AFib.
Practical Example (Path B): The PCP sends the same patient to an electrophysiologist who is a vocal early adopter of your new cardiac ablation catheter.
The treatment path was essentially set in motion by the referrer’s initial decision. If your team is only focused on the end-specialist, you're just competing in an already crowded space, completely missing the invisible hand that guided the patient there in the first place.
For commercial teams, the true meaning of a referring physician is "market-shaper." Their collective referral patterns create the landscape of opportunity for your products, determining which specialists get the chance to use them.
A sales strategy that ignores these upstream clinicians is like trying to change a river’s course by building a dam at its mouth. It’s too late. The real work happens at the source. This dynamic directly impacts how field teams are structured and paid; you can learn more about how medical device rep compensation works and see why targeting the right physicians is so vital.
By identifying and engaging these key referrers, you can start directing patient flow toward the specialists who already champion your technology. That's how you build a real, lasting advantage.
How to See the Invisible Lines of Patient Referrals
You can't just walk into a clinic and see a referral network. These professional relationships aren't something you can physically point to, but they absolutely leave a trail. That trail is buried in the mountain of administrative claims data generated by every single patient visit.
The trick is learning how to read the signs. Think of it like connecting the dots. We can look at billions of anonymized medical and pharmacy claims and start to see patterns emerge. For instance, you might see a claim from a primary care physician (PCP) for a patient, and then, a few weeks later, a claim from a cardiologist for that same patient with a related heart condition. That's a strong signal—a breadcrumb leading from one doctor to another.
It's All About Finding Consistent Patterns
Of course, one or two shared patients could just be a coincidence. The real magic happens when you spot these patterns happening over and over again. When you can see a steady stream of patients flowing from one specific doctor to another over time, you've moved beyond a hunch. You've uncovered a real, established referral pathway.
Even official bodies like the Centers for Medicare and Medicaid Services (CMS) use this logic. They have their own threshold for what constitutes a formal referral relationship in their data. To them, it’s not official until they see a pattern involving at least 11 different patients moving between two providers within a single year.
This is how a referral network stops being a fuzzy concept and becomes a concrete map. You can suddenly see the major highways and quiet backroads that patients travel on their way to a specialist. For commercial teams, this isn't just interesting—it's a roadmap for a much smarter targeting strategy.
It's also worth noting that sometimes the referral source is captured right at the front desk on modern patient registration forms, giving another clue to these connections.
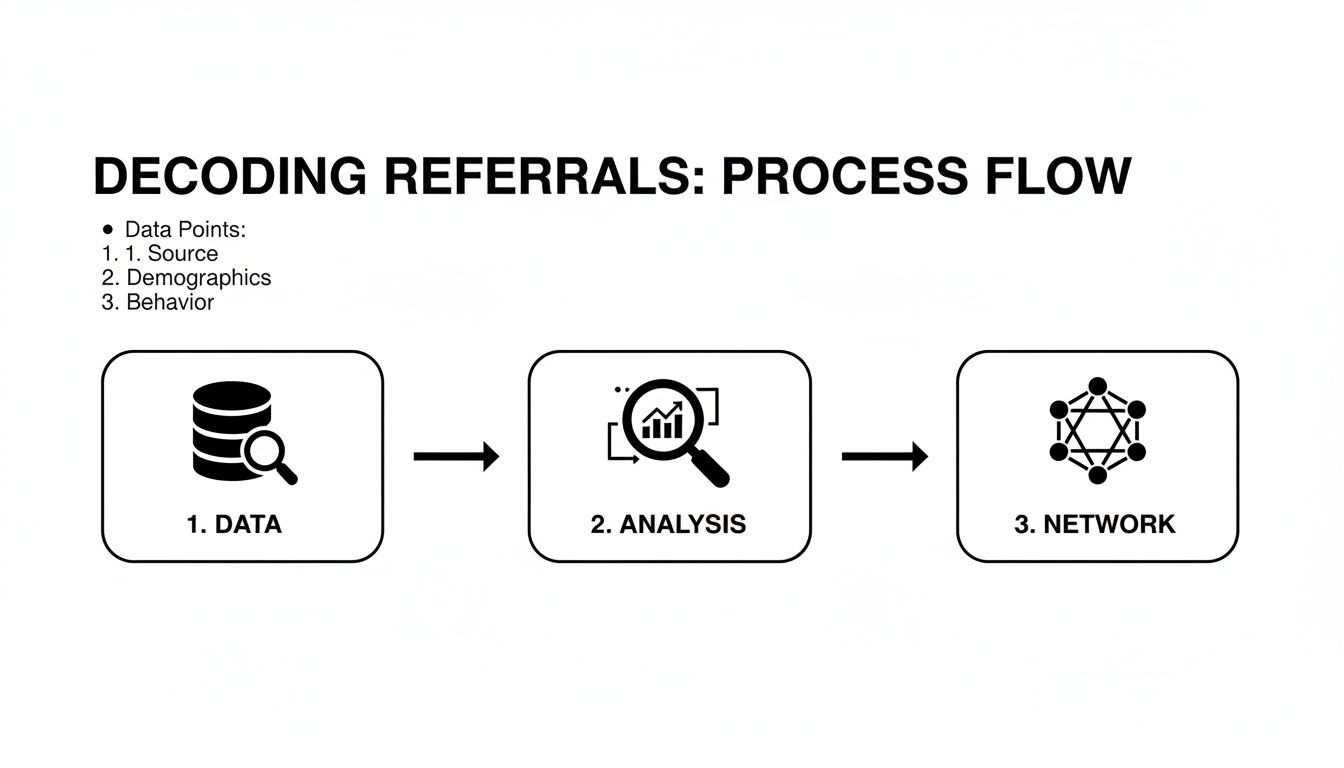
The Specific Signals We Look For
To build this detailed view, we have to sift through the data for very specific clues. When you put these signals together, the full picture of a referral dynamic starts to take shape.
Here’s what really matters:
Timing Between Claims: Are we seeing claims from two different doctors for the same patient within a reasonable window, say 30 to 90 days?
A Logical Diagnostic Story: Do the diagnoses on the claims make sense together? A practical example: an initial visit for chest pain (ICD-10 code R07.9) followed by a specialist visit for coronary artery disease (ICD-10 code I25.10).
Sheer Patient Volume: How many unique patients are flowing between these two providers? This is the ultimate measure of how strong their professional connection truly is.
This process turns a sea of billions of disconnected data points into a clear, usable map. By understanding these connections, your team can stop focusing only on the final prescriber and start engaging the entire network of physicians who guide patient care from the very beginning. For more on how data like this informs strategy, check out our piece on essential benchmarks in healthcare.
How to Turn Referral Data Into Commercial Wins
Knowing what a referring physician is on paper is one thing. Putting that knowledge to work to actually drive commercial success is a completely different ballgame. The real magic happens when you turn raw referral data into a concrete, executable game plan for your field teams. This is how you go from just knowing who the specialists are to actively shaping the market.
It all comes down to a clear, repeatable workflow. You start with a key specialist you want to support and then work backward, uncovering the entire ecosystem of clinicians who feed into their practice.
This process turns a jumble of raw data points into a clear, structured map of the professional networks that truly guide patient care.
A Practical Workflow for Your Commercial Team
Let's walk through a real-world scenario. Imagine you're on a medtech commercial team, and your goal is to find the highest-value referrers who can send more patients to a specialist using your device.
Here’s a step-by-step guide on how that works in practice:
Start with Your Target Specialist: You always begin with a high-value physician who is critical to your business. Let’s say your target is Dr. Evelyn Reed, a top electrophysiologist in a key territory. She’s an expert with your new ablation device, so her success is your success.
Map the Referral Network: Next, you use a healthcare data platform to dig into the medical claims data connected to Dr. Reed. This analysis builds a visual map of her entire referral network, showing you every single physician who has sent her a patient over the past year. You'll quickly see a mix of general cardiologists, internists, and primary care physicians (PCPs).
Filter and Prioritize Referrers: Not all these referring physicians are created equal. This is where you get strategic. You apply filters to this network map to pinpoint the best opportunities for your team to engage. You can segment the list by referral volume, how close they are to Dr. Reed’s practice, and even the specific diagnostic codes they use. This helps you find the PCPs who are consistently sending the most relevant types of patients.
The Actionable Insight: You’ll likely discover something fascinating—that a small group, maybe 20% of the referring physicians, are responsible for 80% of Dr. Reed's patient volume. This is your new high-priority target list.
Integrate and Engage: The final step is to push this prioritized list directly into your CRM. Now your field team has a data-backed roadmap of exactly who to talk to. Their conversations can be much more focused and valuable, educating these high-potential referrers on the conditions Dr. Reed treats and the great outcomes she achieves. When referrers know where to send their patients for the best care, it helps to improve patient experience, which builds trust and keeps those referrals coming.
This methodical approach takes the abstract idea of a "referral network" and makes it a powerful tool for strategic planning and field execution. In many ways, it's a core tactic that shares principles with other complex sales environments, like when you're selling to hospitals and entire health systems.
Answering Your Key Questions About Referring Physicians
Even when you’ve had that “aha!” moment and grasp the importance of referring physicians, a host of practical questions usually follows. You start thinking about the real-world complexities—navigating referral networks, staying on the right side of compliance, and handling data privacy.
Let's dig into the most common questions we hear from life sciences teams. The goal here is to give you clear, straightforward answers that help you build a smarter and, crucially, a more compliant engagement strategy.
What Is the Difference Between a Referring Physician and a PCP?
This is probably the most common point of confusion, and it’s a critical one to get right. While many Primary Care Physicians (PCPs) are indeed referring physicians, it's a huge mistake to think the terms are interchangeable.
The key difference is function versus specialty. "PCP" is a job title, a medical specialty like family medicine or internal medicine. In contrast, "referring physician" is a role someone plays—it describes an action. Any physician, no matter their specialty, steps into the role of a referring physician the moment they send a patient to another provider.
Here's a practical example to illustrate:
A PCP suspects a patient has complex heart disease and sends them to a cardiologist. In this interaction, the PCP is the referring physician.
But it doesn't stop there. That cardiologist might diagnose a specific arrhythmia and then refer the same patient to an electrophysiologist for a specialized procedure. In that next step, the cardiologist is now acting as the referring physician.
For commercial teams, this is a game-changer. It means you have to look past a doctor’s listed specialty and zero in on their actual referral activity. This is how you uncover the true influencers who are directing patient care, regardless of the title on their door.
How Does Stark Law Affect Engagement With Referring Physicians?
When it comes to engaging with any healthcare professional, compliance is everything. This is especially true for referring physicians, where federal laws like the Stark Law and the Anti-Kickback Statute (AKS) set firm boundaries.
At their core, these laws prohibit giving any kind of "thing of value"—be it cash, gifts, or lavish dinners—as a reward for patient referrals if those patients are covered by federal programs like Medicare or Medicaid. The penalties for getting this wrong are severe, including massive fines and being barred from federal programs entirely.
Key Compliance Takeaway: Your entire engagement strategy must be built on legitimate, non-referral-based reasons. You can and should interact with these physicians, but the purpose must always be for legitimate services at Fair Market Value (FMV), like providing medical education, product training, or engaging them as genuine consultants.
When you use data to find physicians who refer a high volume of relevant patients, your goal isn't to reward them for those referrals. It's to educate and support them. This is why using a data platform with built-in compliance guardrails isn’t just a good idea—it’s essential.
Can I See Which Specific Patients Were Referred?
Let’s be crystal clear on this one: an emphatic no. The Health Insurance Portability and Accountability Act (HIPAA) ensures that all patient-level data is completely protected. Before any of it can be used for commercial analysis, it is fully de-identified. You will never, ever see a patient’s name, address, or any other personal information.
Healthcare intelligence platforms are designed to work with this de-identified data. They allow you to spot statistical patterns and map connections between doctors without ever crossing the line into private patient information.
So, here’s what you can see:
Provider A sent a certain volume of patients...
...to Provider B...
...within a specific timeframe...
...for a particular diagnosis or procedure code.
The entire focus is on understanding the professional relationship between clinicians and the total flow of patients between them. You’re mapping the clinical pathways, not tracking individuals.
How Often Should I Analyze Referral Networks?
Referral networks aren't set in stone. They are living, breathing ecosystems that are in constant flux. Doctors move, practices get acquired, and insurance networks change their coverage. A referral map that was perfectly accurate six months ago could be misleading today.
Because of this, the best practice is to refresh your referral network analysis on a quarterly basis.
This rhythm allows your team to:
Anticipate and react to major market shifts.
Spot emerging key opinion leaders and new sources of referrals.
Notice when important referral relationships start to fade.
Fine-tune your field team’s territories and targeting priorities.
Relying on old data is like using an old map—you’re bound to get lost. A platform built on continuously updated claims data ensures your strategy is grounded in today’s market reality, giving you a serious competitive advantage.
Ready to stop guessing and start seeing the real connections that drive your market? G LNK provides the most comprehensive view of referral networks, helping you identify, prioritize, and engage the physicians who matter most. Explore how our platform can transform your commercial strategy and uncover hidden opportunities by visiting https://www.glnkco.com.
People also read

Mastering selling to hospitals: A 2026 Playbook for MedTech
Mar 11, 2026

How Much Do Medical Device Reps Make in 2026?
Mar 12, 2026
What Is Medical Affairs and Why Does It Matters in Pharma
Mar 16, 2026
Decoding the Average Medical Sales Salary in 2026
Mar 15, 2026
Unlock benchmarks in healthcare: A data-driven strategy guide
Mar 13, 2026